Lateral Lumbar Interbody Fusion (LLIF)
Lateral Lumbar Interbody Fusion (LLIF) is a minimally invasive surgical procedure used to treat various conditions affecting the lumbar spine, such as degenerative disc disease, spondylolisthesis, and scoliosis. This procedure involves accessing the spine from the side (lateral approach) to remove a damaged disc and insert an interbody cage, which helps stabilize the spine and promote fusion between vertebrae.
Why Choose LLIF?
LLIF is often chosen for its minimally invasive nature, which typically results in less muscle disruption, reduced blood loss, and quicker recovery times compared to traditional open spinal surgeries. The lateral approach allows for the placement of larger interbody cages, which provide better support and alignment of the spine, promoting successful fusion.
What Happens During LLIF Surgery?
Preparation
Hospital Admission: You will be admitted to the hospital on the day of surgery. Fasting is required before the procedure, as directed by your anaesthetist.
Anaesthesia: The surgery is performed under general anesthesia, ensuring you are asleep and pain-free throughout the procedure.
Surgical Approach
Patient Positioning: You will be positioned on your side (lateral decubitus position), or possibly on your stomach (prone) to allow A/Prof Buckland to access the lumbar spine from the side of your body.
Incision: A small incision is made on the side of your abdomen, and A/Prof Buckland carefully dissects between the abdominal muscles, abdomen and psoas muscle to reach the spine. A specialized retractor system is used to create a working space and visualize the surgical area without cutting through the major muscles of the back.
Disc Removal and Preparation for Fusion
Exposing the Disc Space: The affected disc is exposed by retracting the surrounding tissues. A/Prof Buckland then removes the damaged or degenerated disc, which allows the disc to be distracted to restore the disc height.
Preparation for Fusion: The disc space is thoroughly cleaned and bony surfaces prepared for the insertion of the interbody cage.
Insertion of the Interbody Cage and Bone Graft
Interbody Cage Placement: A cage filled with bone graft material (either from your body, a donor, or synthetic) is inserted into the empty disc space. This cage helps to restore disc height, maintain spinal alignment, and promote solid fusion between the vertebrae.
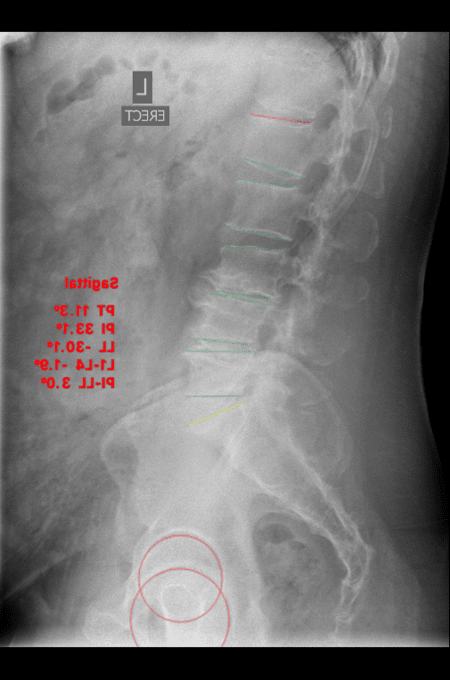
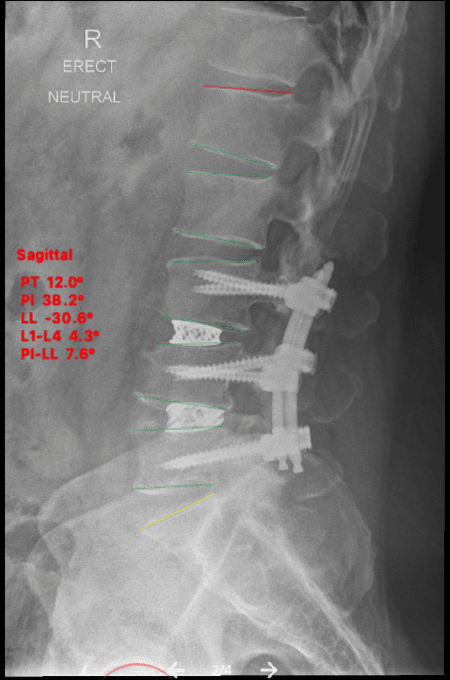
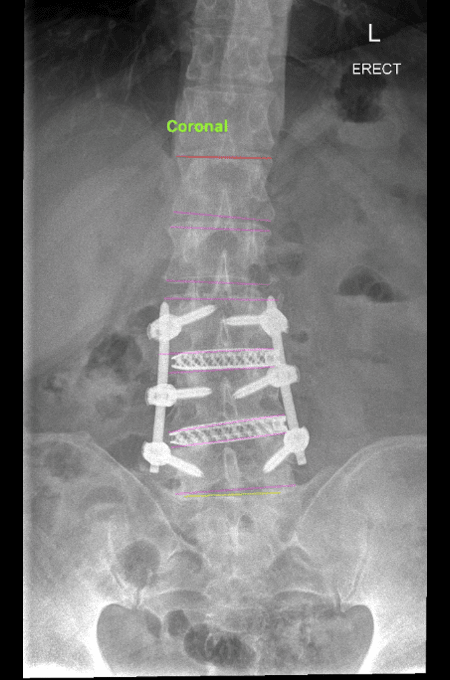
X-ray Verification: Intraoperative X-rays are taken to confirm the correct placement of the cage and ensure the spine is properly aligned.
Supplementary Fixation (if needed)
Typically, fixation with screws and rods may be added through a posterior (back) approach to provide extra stability and ensure proper alignment and increase the rates of fusion.
Closure
The incision is closed with sutures, and a sterile dressing is applied to protect the wound.
Postoperative Care and Recovery
Hospital Stay
Most patients stay in the hospital for 1-2 days following LLIF surgery and are discharged home, depending on the extent of the surgery and their recovery progress.
Pain Management
Pain is managed with medications, and early mobilization is encouraged to reduce the risk of complications such as blood clots or pneumonia. The lateral approach typically results in less postoperative pain compared to traditional back surgeries due to the avoidance of cutting through the back muscles. Groin and thigh pain may occur after surgery, and typically resolves in the first 3-4 weeks after surgery.
Outpatient Rehabilitation
Physiotherapy: A tailored outpatient rehabilitation program will begin shortly after surgery, focusing on restoring strength, flexibility, and proper body mechanics.
Activity Restrictions: Patients should avoid heavy lifting, bending, and twisting for at least 3 months after surgery. A gradual return to normal activities will be guided by A/Prof Buckland’s team.
Follow-up
Regular follow-up appointments will be scheduled to monitor the healing process, assess the success of the fusion, and adjust your rehabilitation plan as needed.
Risks and Complications
As with any surgery, there are potential risks, including:
- Infection: There is a small risk of infection at the surgical site.
- Bleeding: Excessive bleeding during or after surgery is possible but uncommon, and occasionally requires a blood tranfusion.
- Nerve Injury: There is a risk of injury to the spinal nerves or surrounding nerves, including the lumbar plexus, which could result in quadriceps weakness, numbness, or other neurological symptoms. A/Prof Buckland uses nerve monitoring throughout the procedure to minimise this risk. The risk of quadriceps weakness is 1.2%, of which only 0.4% are present at 1 year after surgery1.
- Non-Union: In some cases, the bones may not fuse as expected, potentially requiring additional surgery.
- Groin and thigh Pain: Occurs in the first 3-4 weeks after surgery due to retraction of the psoas muscle (hip flexor). Occasionally (6% of people), this may be associated with more severe pain and sensitivity. This is typically self limiting, and persistent groin and thigh pain is present in <1% of patients at 1 year post-surgery1.
Results of LLIF Surgery
Most patients have significant improvements in pain and function as a result of LLIF surgery. Learn more about A/Prof Buckland’s results of 1-2 level lumbar fusion surgery, complex and revision lumbar fusion, and adult spinal deformity correction surgery.
References:
- Lateral lumbar interbody fusion at L4-L5 has a low rate of complications in appropriately selected patients when using a standardized surgical technique. Buckland AJ, Huynh NV, Menezes CM, Cheng I, Kwon B, Protopsaltis T, Braly BA, Thomas JA.Bone Joint J. 2024 Jan 1;106-B(1):53-61. doi: 10.1302/0301-620X.106B1.BJJ-2023-0693.R2.PMID: 38164083