Hybrid ACDF & Cervical Disc Replacement (CDR)
Hybrid ACDF/CDR is a type of spine surgery that combines two different procedures: Anterior Cervical Discectomy and Fusion (ACDF) and Cervical Disc Replacement (CDR). The surgery is designed to relieve pain, weakness and/or numbness caused by compressed nerve or spinal cord in your neck. The aim of the surgery is to relieve pressure from the nerve and/or spinal cord in your neck to relieve pain and improve function, with the view to get you back to doing what you love.
Here’s a simple explanation:
- ACDF (Anterior Cervical Discectomy and Fusion): This is a surgery where A/Prof Buckland removes a damaged disc from your neck and then fuses the bones above and below that disc together. This fusion stabilizes the spine in that area but makes it less flexible.
- CDR (Cervical Disc Replacement): This procedure also involves removing a damaged disc, but instead of fusing the bones together, A/Prof Buckland replaces the disc with an artificial one. This artificial disc allows the spine to maintain more of its natural movement and flexibility.
- Hybrid Approach: Sometimes, a patient may have multiple damaged discs, but not all of them require the same treatment. In a hybrid ACDF/CDR surgery, the surgeon uses ACDF on one or more discs and CDR on others. For example, if you have two problematic discs, A/Prof Buckland may remove and fuse one disc (ACDF) and replace the other with an artificial disc (CDR).
Why Choose a Hybrid Approach?
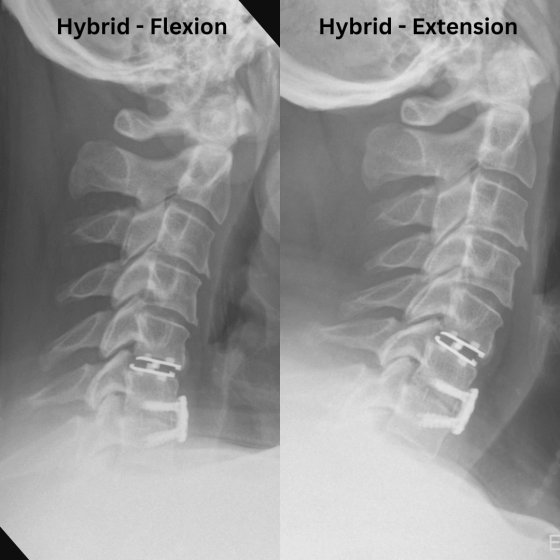
- Best of Both Worlds: The hybrid approach combines the stability of ACDF where it’s most needed with the flexibility of CDR, which can help maintain more natural movement in the neck.
- Customized Treatment: It allows the surgeon to tailor the surgery to the specific needs of each damaged disc, providing the most appropriate treatment for each area of the spine.
- Alternative to 2-Level CDR: Currently in Australia, Medicare does not provide reimbursement for 2- or more levels of Cervical Disc Replacement, but will allow Hybrid ACDF/CDR to treat multilevel disc problems.
Which Disc is Fused and Which is Replaced?
There is not a ‘one rule for all’ on this question. Sometimes the upper disc is replaced and the lower disc fused, and vice versa. Typically the disc that is more damaged (lost most height), or that has associated arthritis in the facet joints (joints at the back of the neck) is the one that is chosen to be fused. A/Prof Buckland makes this decision by his clinical judgement preoperatively and will discuss this detail with you.
Surgical Approach
A small (@ 1 inch) incision is made at the front of the neck. The cervical spine is accessed by gently dissecting between the tissues of the neck without dividing them, and they are gently retracted to allow direct visualisation of the involved discs.
Removing the Damaged Discs
After confirming the correct disc levels, the damaged discs that are causing your symptoms are removed under high powered microscopic magnification. This step is crucial because the damaged disc is often the source of nerve compression and pain.
Relieve Compression from the Nerve and/or Spinal Cord
Using high powered microscopic magnification, the spinal cord and exiting nerves are visualised and freed up from any compression by disc fragments or bone spurs.
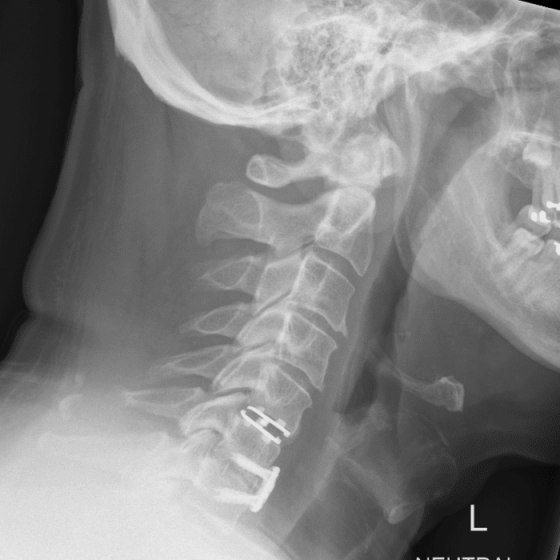
Inserting an Artificial Disc
After the damaged disc is removed, it’s replaced with an artificial disc. This new disc is made of durable metal and plastic and is designed to mimic the natural movement of your spine. The disc is sized appropriately for each person. The artificial disc allows your neck to maintain its flexibility.
Inserting a Cage
After the other disc is removed, it is replaced with a spacer called a ‘cage’. This cage is made of durable metal or plastic and is designed to maintain the disc height to keep pressure off the adjacent nerves as they exit the spine. The cage is filled with bone graft (or bone graft substitute), which allows the vertebrae on each side of the cage to fuse together, forming a column of bone through- and around the cage. The cage is sized appropriately for each person. The artificial disc allows your neck to maintain its flexibility.
Placement of Plate and/or Screws
In order to provide the optimal environment for obtaining fusion, a low-profile plate and/or screws are used to secure the adjacent vertebrae together to prevent movement between them and provide stability to prevent cage migration. The plate and/or screws are only placed at the level of the cage (fused level), but not at the level of the disc replacement.
Recovery
After the surgery, most people spend one night in the hospital. Recovery times vary, but most patients have a resolution of their nerve pain immediately. Most people note some minor issues with swallowing over the first few days after surgery, and the neck may feel tight for the first 3-4 weeks. A soft collar is provided for comfort, but we encourage you to remove the collar and move the neck as comfortable. Avoidance of strenuous physical activities such as lifting and overhead activities is required postoperatively to ensure the implant bonds securely. A/Prof Buckland’s team provides specific postoperative instructions.